
Since the beginning of the COVID-19 pandemic, key elements of hospital operations such as managing inpatient bed capacity, and access to ventilators and PPE have taken center stage. The general public got a crash course on what hospitals need in order to function successfully when disaster hits, and daily news and discussions were centered around ICU bed capacity as cases accelerated across the country.
The nightmarish predictions and reality led to the development of creative measures to help meet such catastrophic needs such as popup temporary screening and triage sites, non-medical and medical spaces being repurposed for COVID units, increased patient transfers to hospitals that had more space, and mathematical models to predict upcoming numbers of new COVID-19 cases.
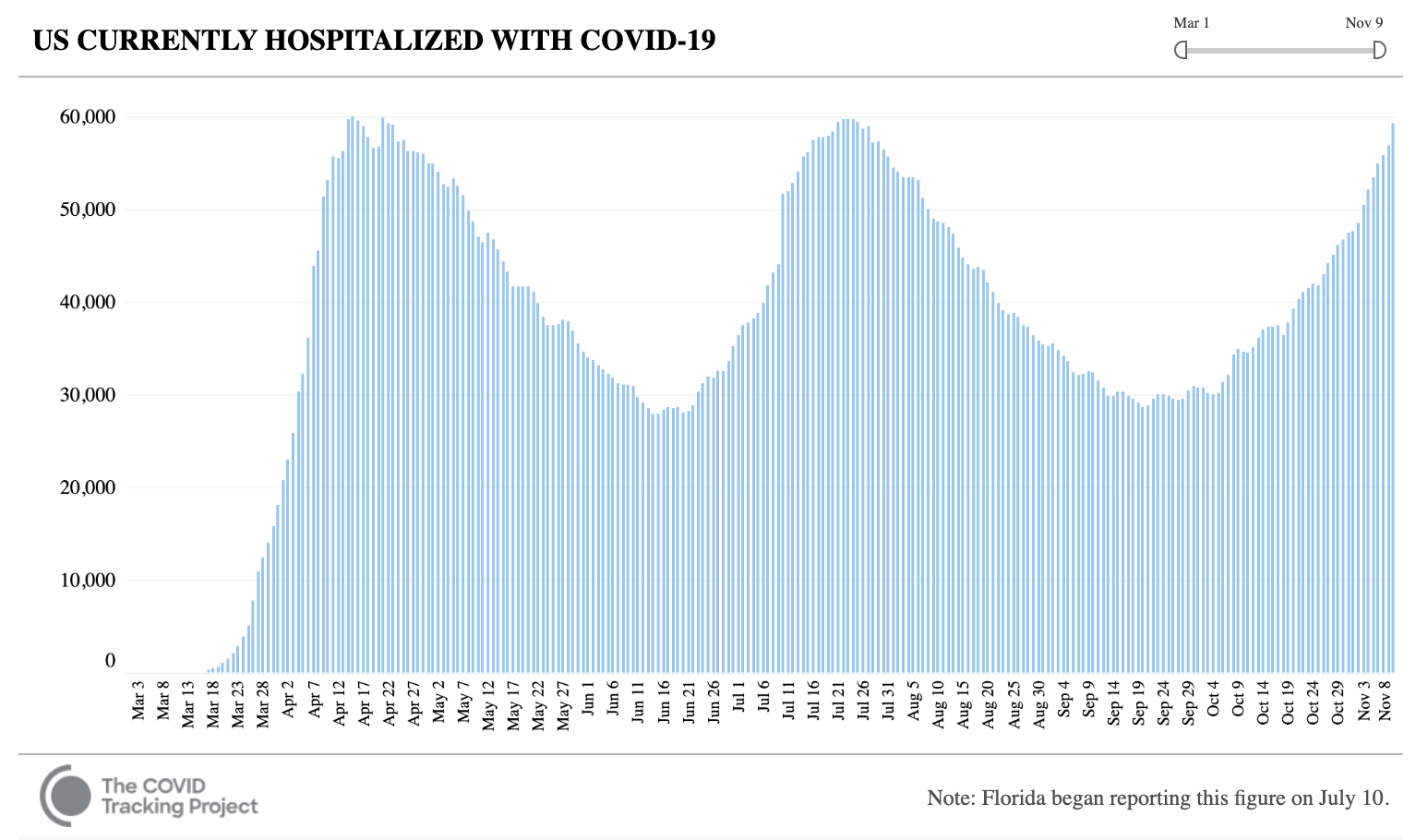
With the latest surge of COVID-19 cases (see figure 1), some states have or will begin opening up field hospitals (Wisconsin, Texas) while others are considering transfers to other locations (both in and out-of-state), and even the concept of ‘rationing care’ has surfaced.
This public health crisis intensified what happens when hospitals and healthcare providers run out of the right space and resources. As alarming as it has been to watch this play out, the reality is that these capacity and resource challenges are not unique to the pandemic; they happen often in hospitals across the country, just on a different scale. Bed capacity is something hospital leaders manage every day – only 1 of 3 hospital beds are available on any given day in the U.S., per research by the Robert Wood Johnson Foundation 2. Of course, there’s further variation when looking at urban versus rural regions. Many systems are forced to go on ‘diversion’ (patients will literally be re-routed to other hospitals) when the reality is that they are bursting at the seams.
Clearly, the pandemic has been devastating, yet it has (finally) propelled healthcare toward innovation and adoption of technology that was much needed in order to improve access to and utilization of quality and cost-effective care. Although the waves continue, organizations are starting to answer the following questions: What newly applied practices do we keep from the pandemic moving forward as we head into additional COVID-19 waves and the flu season? Can we more vigorously apply lessons of the past and present to tackle our future needs? Are our incentives aligned such that the solutions we pursue can be sustained and still “keep the lights on”?
Delayed access to care and, even worse, lack of access to care, have been among the most devastating consequences of the capacity crises during the pandemic. Though many of our systems started to transition back to their usual state of affairs by July, other factors in addition to the current surge continued to highlight the ongoing need for creating and sustaining ‘good patient flow’.
Under “normal” circumstances, daily chaos is anticipated and actually expected, as hospitals experience the inability to move patients from the emergency room (ER) or operating room (OR) due to a “lack of beds” in the hospital. While this inevitably requires hospital leadership to ‘do something’ about it, it is a scenario that plays repeatedly throughout the day, every day.
The chaos that comes from the lack of visibility into available beds, let alone appropriately available levels of care, can have negative downstream impacts not only on the patients but also on the frontline staff. Patients are subject to suffering the consequences of inappropriate levels of care, poor clinical outcomes, and/or poor provider/patient experiences.3 Staff are subject to the stress of caring for patients for whom they are not necessarily appropriately trained to care for.
Despite the known implications, this lose:lose cycle continues. These “risks” plus the impact of significant revenue losses from the pandemic highlight the urgent need to address poor, inefficient patient throughput. We are at a critical point where healthcare systems must do what is necessary to improve existing practices when it comes to bed management.
Some examples of improvement include:
– Create machine learning models for all locations and patient movements within the hospital, and adjust space and schedules accordingly
– Place patients using sophisticated demand-supply model
– Make data-driven internal transfer decisions
– Right-Sized unit capacity
– Look hard at the degree of specialization to pool capacity where possible
– Smooth the patient flow from the OR
Take a magnifying glass to internal operational workflows – Identify practices that work, areas where support is needed, especially when it comes to discharge planning, and whether or not there are financial implications.
– Improve provider workflow
– Don’t let “a dime hold up a dollar”: take a hard look at staffing, hours of operations, and transportation
– Use predictive discharge planning to focus on case teams and social services
Identify clinical workup that can be prioritized according to disposition, treat outpatient setting
– Prioritize discharge patients in queues for labs/clinical procedures
– Transition some procedures to outpatient
With the recent surge of COVID-19 cases across the nation and the impending flu season, hospitalizations will continue to rise. Although health systems will be able to resurface earlier crafted emergency plans from previous surges, set up incident command centers more quickly, and have a more stable supply inventory, they will likely continue to manage their bed capacity through a very manual process. It is imperative that we start to do things differently to achieve better outcomes!
Implementing operational change and deploying new but proven technologies that incorporate both artificial intelligence and lean principles will increase patient access, improve provider, patient, and staff experience, and, of course, smooth inpatient capacity. As a result, terms such as chaos and crisis can, in time, become things of the past.
References:
1. The Covid Tracking Project Nov. 10, 2020. Retrieved from https://covidtracking.com/data/charts/us-currently-hospitalized
2. Blavin F., (March 1, 2020). Hospital Readiness for Covid-19: Analysis of Bed Capacity and How It Varies Cross The Country The Robert Wood Johnson Foundation. https://www.rwjf.org/en/library/research/2020/03/hospital-readiness-for-covid19-analysis-of-bed-capacity-and-how-it-varies-across-the-country.html
3. Mohr et al., Boarding of Critically Ill Patients in the Emergency Department. Critical Care Medicine 2020; 48(8): 1180–1187
4. Agrawal S., Giridharadas M., (2020) Better Healthcare Through Math: Bending the Access and Cost Curves. Forbes, Inc.
About Dr. Pallabi Sanyal-Dey
Dr. Pallabi Sanyal-Dey is the director of client services for ‘iQueue for Beds’ Product at LeanTaaS, a Silicon Valley software innovator that increases patient access and transforms operational performance for more than 300 hospitals across the U.S. Dr. Sanyal-Dey is also a visiting associate professor of medicine, providing career mentorship to trainees at the University of California, San Francisco Medical Center (UCSF) where she attends on the internal medicine inpatient teaching service. Prior to joining LeanTaaS, Dr. Sanyal-Dey was at UCSF, as an assistant clinical professor and an academic hospitalist at Zuckerberg San Francisco General Hospital where she directed clinical operations for the Division of Hospital Medicine, and oversaw the faculty inpatient services.