Can virtual healthcare close the care gaps? Dr. Leslie Saxon gives us a glimpse of what’s to come via the latest in telehealth technology.
 Virtual care is quickly becoming a tangible reality. All over the word, fingertips are tapping onto screens and into data streams, leaving digital footprints in their wake. But where is this trail of telecommunications leading us? According to Dr. Leslie Saxon, we are headed for real progress in creating access to healthcare by plugging deeper into its potential.
Virtual care is quickly becoming a tangible reality. All over the word, fingertips are tapping onto screens and into data streams, leaving digital footprints in their wake. But where is this trail of telecommunications leading us? According to Dr. Leslie Saxon, we are headed for real progress in creating access to healthcare by plugging deeper into its potential.
In January, Saxon who is the executive director of the University of Southern California’s (USC’s) Center for Body Computing (CBC), announced a partnership with eight foundational partners to launch its Virtual Care Clinic (VCC). The digital healthcare model utilizes a variety of technologies, including mobile apps, wearable sensors, virtual human health care providers, augmented virtual reality (AR/VR), data collection, analytics and artificial intelligence using digital communication tools allowing patient’s anywhere to access medical care and content.
The clinic will demonstrate how patients can handle their health matters without ever leaving their homes. To get a better understanding of how this amalgam of new technologies will achieve that task, we asked Saxon for what’s to come from the launch of the clinic—along with how this new-found technology will create greater touchpoints through digital means for those in need of healthcare services.
Q
Let’s start off by talking about how this initiative is different from some of the other telehealth initiatives we are seeing out there right now: Unlike traditional remote conferencing with doctors, we are talking about taking virtual readings through equipment and apps, can you further explain what a virtual visit might look like and what types of technology are involved?
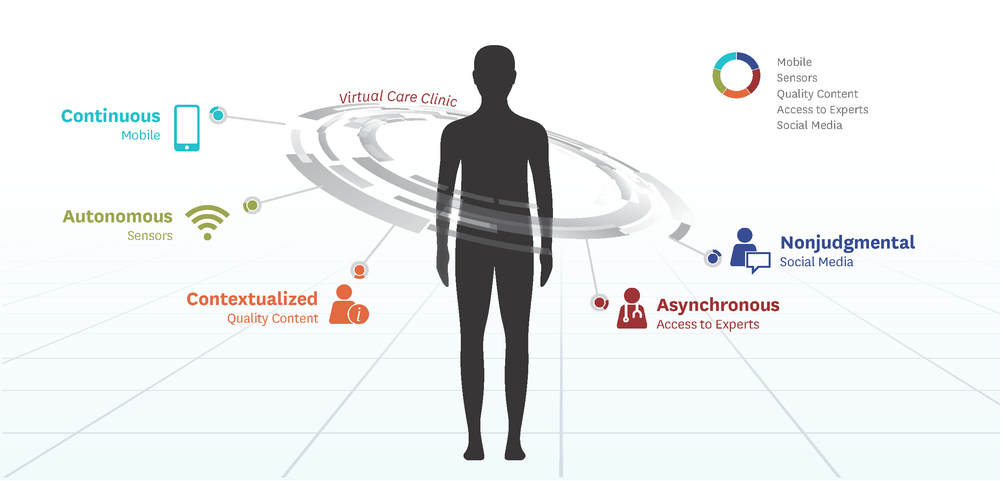
Sure. With the creation of the Virtual Care Clinic (VCC), what we are building is a continuous model of healthcare that is focused on the patient and is on-demand. That means continuous diagnostics with wireless sensors and fully leveraging the sensors and coprocessors in the phone to provide context to the healthcare data (like geolocation, photos, videos, HealthKit). The other attribute of this system is the use of the virtual-human physician.
We are creating virtual-human representations of USC’s physician experts that will be available to patients on demand to answer questions. We are partnering with our Virtual Care Clinic’s foundational members, like Dr. Evidence, to deliver the best medical evidence to VCC patients that is on demand and tailored specifically for their condition. This requires a creative engagement of the patient and new types of data visualization and analytics. Eventually, we would like our virtual-human doctors to be capable of conceptual thinking, but this will require time. Our digital platform will be built so that rapid iteration is possible, and this work is in collaboration with our digital platform partner, Medable.
Another partner, Proteus Digital Health has created an incredibly powerful platform for tracking medication adherence and patient activity that fully engages the patient and care providers in a digital collaboration and discovery process with their physicians. This system includes the ability to identify the relationship between activity or other vital signs and medication adherence. VSP Global, the world’s largest insurer of eye care, is partnering with us to deliver the best-in-breed health and wellness sensing solutions over eye and other healthcare.
Q
There’s no question that telehealth is expected to blossom and grow substantially over the next few years, but how is this kind of service delivery going to adequately replace human interaction? Can fully sufficient and thorough healthcare services be delivered via virtual means?
There is no replacement for human interaction, but research performed at the VCC location, USC’s Institute of Creative Technologies, has shown that people often disclose more to virtual human agents than to actual human care providers. This makes sense because virtual-human interaction occurs on the user’s own schedule and is devoid of judgment. The truth is that with widespread adoption of the electronic medical record, and the additional compliance burden that the Affordable Care Act places on physicians, most U.S. physicians spend between 40 to 60 percent of their working day documenting in the electronic medical record to fulfill compliance mandates—much of this impinges on time spent with patients and involves multiple, mundane and repetitive tasks.
Physicians need to be dis-intermediated from many of these tasks to do what they do best: take care of patients. Our VCC model provides unprecedented efficiencies for patients and physicians and includes the communities that surround both groups, so that communication can flow freely. I view the VCC as the 99 percent of the patient care in the future and the traditional bricks and mortar patient care facilities as the 1 percent.
Q
In every experimental launch there seems to be a share of lessons learned. What do you think will be the most teachable aspects of running this clinic? What are some of the expected challenges you think this kind of interaction will naturally produce, and what’s the protocol for overcoming some of those challenges?
The VCC is incredibly ambitious in its goals to deliver a universal healthcare system. Currently, we are challenging ourselves to create the early models of virtual care by bringing together (very frequently) the multidisciplinary group of creatives (patients, clinicians, technologists, care providers, drug and device manufacturers, and regulators and analytic experts) to bring the best-in- breed service models, medical content, and care and user experience for the patient and the physician.
Many of the software tools we are using are untested in this context, and it’s incumbent upon us to show that we are improving on the status quo, saving costs, and advancing medical care and research. Our foundational member, Karten Design, has a term ‘fail forward quickly’ when testing new prototypes, that’s what we aim to do and we will also learn in partnership with our patients.
Q
Certainly this kind of project serves a blueprint for a larger initiative, does it not? Is this a thumbnail of what will be a much bigger transformation when we think about telehealth? Is this kind of care model realistically scalable?
Exactly, there are not enough medical experts to provide top-drawer healthcare globally. In this model everyone wins. Expert physicians, that are the greatest assets to current health systems, can be leveraged across large populations and that creates unprecedented access. When brick and mortar facilities need to build where there are none, they can be targeted to those needs that can’t be addressed virtually. Moreover, patients can be much more accurately triaged to appropriate facilities. These efficiencies will create much more opportunity for discovery and advancements in diagnosis and treatments. The ability to provide highly engaging medical education over smartphones, using video and other methods that don’t even require literacy to reach populations is, in itself, an enormous opportunity that could have a profound impact on health and health habits in developed and developing nations.
Q
As you mentioned, one of the critical aspects of this kind of care is to create greater access to the underserved. Do you foresee virtual clinics being built to reach those underserved communities in the future? Will they work to complement or in competitive with providers trying to establish more meaningful population health management services?
It’s ironic that the growth of concierge, cash-pay medicine around the globe is available only as a premium service to those with the most expendable income because indigent populations are the prime targets for the highest level of medical service and care. This is because they are also facing challenges like unstable housing, food supply, or the possibility of deportation. These people cannot leave their jobs to wait hours in a publically-funded clinic or pharmacy for their medication and may not share a common language with their providers. The one asset that many of these populations have is an Internet-connected phone that can be used to provide many of these services.
Q
What kinds of healthcare services do you think are better suited for virtual-service model? What are some types where you think traditional methods will continue to require traditional heath delivery models?
Medical content and many medical diagnostics can be provided virtually with technologies that are already out there. Serious trauma or other interventional procedures, some diagnostics and very serious conditions like kidney failure requiring hemodialysis or organ transplant will always require hospitalizations.
Q
I can see how virtual clinics could deliver acute, non-emergency care quite effectively. But do you really think that disease management and prevention will be effective via technology, especially when access to technology is critical. For example, a person may visit a virtual clinic once for a problem, but to monitor a problem or manage it with their physician; that may be difficult for those who don’t have access to mobile devices regularly. Thoughts?
I guess I see the main problems with these two systems we are talking about as problems of interoperability and understanding how to transmit and translate data from one system to another. I’m certain that all of the virtual solutions will be centered on the patient who will be the hub of information sharing. The thing that we don’t want to create is the same type of digital fragmentation of services and information that cripples traditional medical care and makes it extraordinarily difficult to be a patient.
Q
For providers, is there a learning curve to conquer here when we talk about delivering care via virtual technology, or is it pretty intuitive?
I can tell you that doctors desperately need to get back to do doing what they are trained to do and to reach more patients than they currently do. Our job is to show them that these solutions make them better and more efficient and are not associated with great risk.
Q
In the Wake of CMS’ new ACO model guidelines and its embracement of telehealth, do you think that will accelerate the pace of telehealth-service adoption? What should a provider interested in providing telehealth services consider before embarking on such a task?
If we look at the number of businesses that have been disrupted by digital (like music, media, retail, entertainment, finance, real estate, etc.), it seems pretty clear that large populations choose the convenience and autonomy that digital access providers. I view ACO’s as accelerators to adoption of VCC model for traditional medical systems, because they are now dealing with a fixed amount of money to care for complex conditions and that motivates much-needed change and focus on digital, patient-facing products and services.
Q
What do you think will be the greatest benefit of practicing medicine this way? What will be the biggest drawback?
My brother, who is a movie producer, says that medical care is like a horror movie for most patients…the movie shot that asks, “what’s behind the closed door?” The VCC is trying to change the narrative for patients through unprecedented access and education around health and disease. We hope to create knowledge and community that tells a new narrative where patients can be the heroes of their healthcare journey or for their loved ones.
I guess my greatest fear is that someone will figure out a way to exploit people at their most vulnerable, because we will have huge tranches of patient data that are always going to be vulnerable no matter how careful we are.
Q
What are you most enthusiastic about as you are newly embarked on this process?
I think we have the potential to make exponential leaps into our understanding of the transition from health to disease because we’ll be collecting data on large populations over people’s lifespans.
Q
What’s the key take away here for our readers? What should we think of when we think of USC’s launch?
Think of a medical care and content model that is at your fingertips, which allows you to manage your own and your loved one’s care, with less cost and less friction than what exists now. Imagine a continuous healthcare guardian that predicts illness and allows you to intervene earlier, and with the knowledge you need. Imagine engagement and democracy in healthcare decision-making.